TSRI Researcher Develops New Vaccine to Treat Cocaine Addicts
By Jason Socrates Bardi
A group at TSRI has designed a new vaccine against cocaine
that could become a valuable tool in treating addiction. Principal
investigator Kim Janda and his colleagues in the chemistry
and neuropharmacology departments have synthesized this molecule
and tested its efficacy against cocaine.
Structurally similar to cocaine, this vaccine was successful
in laboratory models—data that is presented in the February
13th issue of the Proceedings of the National Academy of Sciences.
In the mid-1990s, Janda’s group discovered a previous
and similarly potent vaccine.
“[These vaccines] suppress the reinforcing aspects
of the drug,” says Janda. What is most interesting is,
unlike other types of treatment, these vaccines do not interfere
with the neurological targets of the drug, but instead help
the body keep cocaine from ever reaching the brain in the
first place.
The vaccines do this by inducing an active immune response
that creates antibodies against cocaine in the bloodstream.
If an addict later takes a hit, the antibodies will clear
the cocaine from the system.
Clinically, this sort of therapy could be given to people
in treatment programs to aid in their recovery. And, like
most other types of treatment, it will only be useful for
those who want the help.
“This is for people who are who are interested in getting
off the drug,” says Janda. This may be a large market.
Though the epidemic of cocaine addiction has waned somewhat
since its peak in the mid-1980s, the numbers are still alarming.
There are nearly 2 million regular cocaine users in the United
States today, according to the National Institute on Drug
Abuse (NIDA), and cocaine is the leading cause of heart attacks
and strokes for people under 35.
The Drug
Cocaine, which is derived from the leaf of the Erythroxylaceae
coca plant, is a highly potent drug that, as a salt, is either
snorted or dissolved in water and injected directly into the
bloodstream. The salt is also often neutralized to make an
insoluble “free-base” form that is smoked.
Once it is ingested in the bloodstream, the drug crosses
the blood–brain barrier and accumulates rapidly in the
brain. “The brain levels rise very rapidly once cocaine
is taken into the system,” says Janda.
Moreover, the cocaine builds up in the ventral tegmental
area. This area is connected by nerve cells to the nucleus
accumbens, the so-called pleasure center of the brain. There,
the cocaine molecules interfere with the normal regulation
of dopamine by binding to dopamine transporters and blocking
them from recycling the neurotransmitter.
This leads to the build-up of dopamine in the brain’s
pleasure center, which produces a euphoric feeling in the
user—a quick rush that hits seconds after taking the
drug that lasts several minutes.
The psychological effect of this immediate reward is the
basis of the addiction that many cocaine users suffer from.
Compulsive users—addicts—will keep a perceived need
for the effect that will many times confound a recovering
addict’s best efforts to stay clean.
There’s an old truism among intravenous drug addicts
that their first boost—that first snort of coke, shot
of heroin, or puff of crack—was the greatest feeling
they had ever experienced. Many of them will also tell you
that they too often spent their money, their health, their
family, their friends, and their lives to get that feeling
back.
“Many crack addicts will say the same thing,”
says David Smith, founder and medical director of the Haight
Ashbury Free Clinics in San Francisco. “They will tell
you, ‘I took 10,000 hits, one hit at a time,’ always
thinking of the next.”
Smith has run outpatient and residential drug detoxification,
counseling, and substance abuse treatment programs in his
Bay area clinics since 1967. Cocaine abuse is especially problematic
in urban settings like the Bay area, where high numbers of
addicts create large markets—nearly $5 billion a year
nationwide—which only increase the drug’s availability.
1 | 2 |
|

Eli R. Callaway Jr. Chair in Chemistry
and Skaggs Institute for Chemical Biology Professor Kim Janda’s
immunotherapeutic cocaine vaccines are unique among approaches
to drug therapy. In fact, they more closely resemble the treatment
of an infectious disease than a psychological disorder. (Janda,
front, is pictured here with Postdoctoral Fellow Marion Wenz).
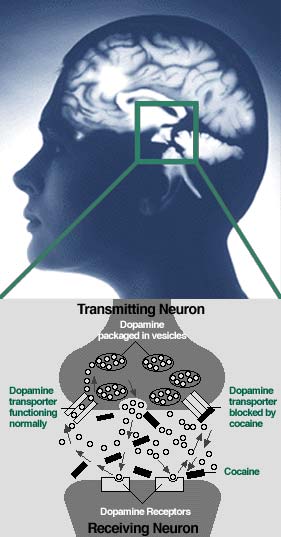
Diagram showing the ventral tegmental
area of the brain and a representation of the synaptic basis
for cocaine highs and addictions. (Picture courtesy of NIDA
and the National Institutes of Health).
|

