

An Eye to the Future
By Mika Ono
Martin Friedlander, professor at The Scripps Research Institute and physician at Scripps Clinic and Green Hospital, has a knack for being at the right place at the right time. Most recently, Friedlander finds himself in the vanguard of one of the hottest topics in medical research—stem cell therapy—as a specialist in one of its most promising therapeutic areas—the eye.
"There's a huge interest in stem cells right now," says Friedlander. "Almost every week I get a call, often about a new stem cell conference or symposium that is being organized. There's a lot of excitement."
The promise of stem cells spring from the fact that they are "pluripotent," in other words they possess the ability to develop into many other distinct cell types, such as nerve, heart, or lung cells. This chameleon-like property holds out the tantalizing possibility of harnessing this ability in the repair of damaged tissue from any number of diseases.
Friedlander's most recent grant—$6 million from the California Institute for Regenerative Medicine (CIRM)—funds research into a new approach to developing treatments for age-related macular degeneration, a common condition that can lead to blindness.
The leading cause of vision loss in Americans over the age of 65, age-related macular degeneration is caused by a loss of cells called retinal pigmented epithelium (RPE), which then leads to a loss of central vision. Vision is lost due to damage to the retina, the "sensory" membrane that lines the eye, contains the rods and cones that capture photons, and signals the brain through the optic nerve.
"The clinical reality is that 6 to 8 percent of people over the age of 75 are legally blind from this disease," notes Friedlander, who sees patients every Wednesday in the clinic in addition to his work in the laboratory.
Although antioxident supplements can slow progression of age-related macular degeneration and some drugs can address the "wet" form of the condition (involving the abnormal growth of new blood vessels), there is currently no treatment that will prevent or reverse the loss of RPE cells and the resulting loss of vision. The need for new treatments is especially acute for the more common "dry" form of the disease (involving degeneration and scarring of the macula, an area near the center of the retina with the greatest visual acuity).
Finding a way to replace these valuable RPE cells could potentially preserve vision, quality of life, and independence for a great many people. But how to accomplish this feat?
Finding a Way
Despite its promise, stem cell therapy is still at an early stage of development, with many unanswered questions and a number of potential pitfalls for the unwary. Friedlander, however, is now hopeful that with further research stem cell therapy can indeed become a reality.
One potential problem that troubled Friedlander about some proposed types of stem cell therapy was tissue rejection, also a major challenge with organ transplantation. Even though the eye is somewhat sealed off from the immune system, Friedlander never warmed to the idea of using stem cells from embryonic tissue for therapeutic purposes, even apart from the ethical controversy involved. "I didn't like the idea of taking cells from somebody else and putting them in the eye," he says.
So when Friedlander first chose to enter the field of stem cell research about 10 years ago, he opted to research the use of a type of stem cell that resides in adult bone marrow. That way, stem cells could be administered to the same individual who generated the cells. While not easy to extract and possessing slightly different properties than embryonic stem cells, the use of bone marrow-derived stem cells did indeed avoid the issue of tissue rejection.
Even better, Friedlander and colleagues showed the cells acted therapeutically. In a series of studies, the group showed the potential of this approach. When the team injected immature white blood cells from bone marrow—myeloid progenitors—into a mouse eye, these cells integrated into the back of an eye that was developing normally. When these stem cells were injected into an eye with an abnormal vasculature (network of blood vessels), they stabilized and prevented deterioration of the eye. In addition to rescuing blood vessels, the cells had a "neurotrophic rescue effect" in which neurons in the eye were saved. Further work described some of the mechanisms of these rescue effects, showing that the progenitor cells migrate to avascular areas of the retina, and once there differentiate into cells called microglia that actively promote vascular repair.
Given the work's potential as a treatment for a range of retinal vascular and degenerative diseases—including diabetic retinopathy, age-related macular degeneration, glaucoma, and retinitis pigmentosa—Friedlander is currently working to move this project "from bench to bedside." Funded by a $17 million grant from the National Eye Institute, Friedlander's group is collaborating with five other Scripps Research labs, those of Laura Crisa, Glen Nemerow, Wolfram Ruf, Gary Siuzdak and Bruce Torbett. Together, the scientists are conducting the extensive pre-clinical work necessary before the technique can be tested in humans.
A New Approach
With the current CIRM grant, however, Friedlander and colleagues are exploring a new and potentially more user-friendly approach.
Instead of harvesting adult stem cells from bone marrow, the scientists are looking at the feasibility of using skin cells—which have the advantage of being easily accessible—as the donor cells. Because these cells do not start out as pluripotent, they must be transformed into stem cells (in this case called "induced pluripotent stem cells" or iPSCs), using chemical and molecular biology techniques, then coaxed from that point to turn into the much-needed RPE cells lost to macular degeneration.
While previous technologies used potentially cancer-causing viruses and animal cell supplements to accomplish this manipulation from skin cell to stem cell, Friedlander hopes to avoid both by the use of new techniques under development by some of his colleagues.
One notable collaborator on the project is Scripps Research Associate Professor Sheng Ding, who recently pioneered a technique to use a chemical and molecular biological approach to inducing cells back to a pluripotent state without the use of viruses (see Cell Stem Cell, April 23, 2009). This development may finally make the development of stem cell therapy from skin or hair cells a practical reality.
Friedlander has a clear vision of what he hopes to accomplish with the CIRM grant work.
"If we are successful, a patient with early signs of age-related macular degeneration could come into his or her ophthalmologist's office and have a skin biopsy performed that could be used to obtain RPE cells," says Friedlander. "Those cells could then be transplanted into that individual's eye at a later date when his or her own RPE begins to degenerate, but before there is visual loss. That's the hope."
A Propitious Start
Friedlander, who earned his Ph.D. from the University of Chicago and his M.D. from State University of New York Downstate Medical Center, first became interested in the field of vision in part because he wanted to combine a career in academics with a one as a clinician.
"My wife [also a physician] convinced me that ophthalmology was the way to go," recalls Friedlander, "because you can do everything from diagnosis to treatment to surgery and medicine. In addition, there aren't a lot of true emergencies like OB-GYN or cardiology, so it's a little more amenable to an academic career."
Significantly, Friedlander also had a head start on an interesting piece of eye-related research.
During medical school and then as a postdoctoral fellow at Rockefeller University, Friedlander worked in the laboratory of Günter Blobel, who went on to win the 1999 Nobel Prize in Physiology or Medicine for his description of the general principles underlying the sorting and targeting of proteins to particular cell compartments and who chairs the Scripps Research Board of Scientific Governors. One key element of this work was the discovery that the protein itself carries the information that specifies its proper destination in the cell with "cellular zip codes" known as topogenic signals.
Friedlander participated in that early research first describing the presence of internal topogenic signals in polytopic membrane proteins like rhodopsin, a protein essential for sight. This project resulted in a paper in the prestigious journal Nature (Friedlander's second, at that early stage of his career) six months after the work began.
"Günter always said I didn't suffer enough," laughs Friedlander.
In his lab today, Friedlander continues to pursue a related line of research, investigating the role that topogenic signals play in targeting visually important polytopic membrane proteins to their proper places in normal and diseased eyes. It appears that when proteins are mutated and display the wrong cellular "zip code," the resulting changes in the eye can lead to such debilitating conditions as retinal and macular degeneration.
Full Circle
In another line of research in his lab, Friedlander is focusing on understanding the growth of new blood vessels ("angiogenesis") and its relationship to a variety of diseases. The abnormal formation of new blood vessels ("neovascularization") is involved in the vast majority of diseases that lead to catastrophic loss of vision. This includes not only age-related macular degeneration, but also retinopathy of prematurity, a significant cause of vision loss in premature children, and diabetic retinopathy, the most common cause of blindness of people ages 20 to 74, according to the American Diabetes Association.
In these cases, the abnormal formation of new blood vessels in the back of the eye appears to be a response to restrictions in blood vessels and insufficient oxygen in the tissue ("ischemia"). But, unlike in the heart or brain, where the extra blood vessels can have a benefit, the new vessels wreak havoc in the eye, leaking fluid and blood and leading to vision loss.
"New blood vessels form as the body's misguided response to the need to bring more blood and oxygen to the back of the eye," says Friedlander.
Current treatments for these eye diseases—such as thermal lasers and anti-angiogenic drugs—are designed to prevent the growth of new vessels or to close, ablate, or remove abnormal vessels. However, this treatment strategy fails to address the underlying cause of the disease—cellular degeneration and lack of oxygen in the tissue.
That's where Friedlander's stem cell research comes in. With it, he has been able to build on years of previous work to take a dramatically different approach to therapy. Instead of destroying blood vessels to control the symptoms of vascular diseases of the eye, stem cell therapy seeks to address the underlying cause of the problem, repairing the cells whose degeneration leads to lack of oxygen and blinding diseases.
Positioned for Success
Friedlander has no regrets about choosing to straddle the worlds of the clinic and the laboratory. He is adamant that his dual role not only makes him a better physician by keeping him current on the latest findings in the field, but also that his work in the lab is constantly informed by the problems he sees patients facing.
"My work in the clinic is so useful to my research that often both the clinically trained (M.D.) and basic science (Ph.D.) fellows in my lab will come over and look at patients," he says. "It's one thing to look at a mouse eye when trying to understand angiogenesis, and it's another to look into the back of a patient's eye with diabetic retinopathy. It brings the meaning of the work to a whole different level. It helps focus."
In addition to the perspective provided by his work in the clinic, Friedlander attributes part of his success to the strong support of funding institutions such as the National Eye Institute, the MacTel Foundation, and CIRM, and the academic freedom and atmosphere of collaboration provided by Scripps Research.
"I'm trained as a basic scientist, but it's really exciting when you can take something from bench to bedside," he says. "That's one great thing about Scripps. As long as I can support my research with grants, I pursue whatever line of investigation I think is worthwhile. It also helps that I have an outstanding group in the lab and tremendously stimulating and interactive colleagues to collaborate with."
Send comments to: mikaono[at]scripps.edu
"I'm trained as a basic scientist, but it's really exciting when you can take something from bench to bedside," says Professor Martin Friedlander.
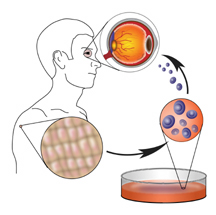
Friedlander hopes that one day a patient with early signs of age-related macular degeneration could have a skin biopsy to obtain cells, which would be transformed into RPE cells and transplanted into that individual's eye to prevent visual loss. (Image by Mary O'Reilly.) Click to enlarge.
